
Menopause Hormones 101 — Part Two Progesterone: the other half of the hormone story

The hormone that calms, protects, and helps you sleep — and often the first to fade.
Welcome back to our Menopause Hormone 101 series. Last time we covered estrogen — the hormone most people associate with menopause. Now it's time for progesterone, estrogen's essential partner. Together, these two hormones are produced by the ovaries throughout your reproductive years: estrogen regulates the menstrual cycle and supports many body systems, while progesterone prepares the uterus for pregnancy, promotes restful sleep, calms the nervous system, and supports bone health.
Why progesterone matters during perimenopause and menopause
Many women are surprised to learn that progesterone is typically the first hormone to decline during perimenopause — the transitional years leading up to menopause, often beginning in the mid-to-late 40s. This decline happens because ovulation becomes less predictable, and since progesterone is produced after ovulation, fewer ovulatory cycles mean lower progesterone levels — even when estrogen remains normal or is temporarily elevated.
This imbalance between estrogen and progesterone may contribute to many common perimenopausal symptoms:
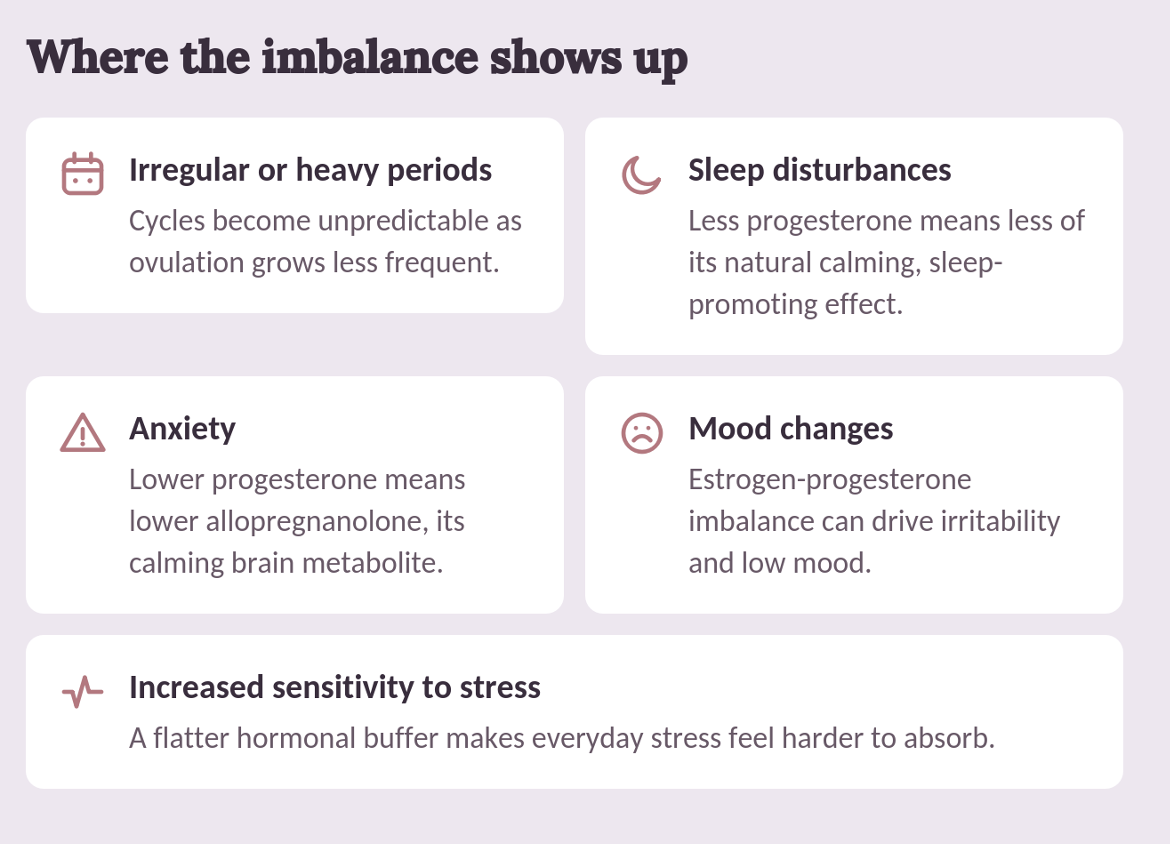
By menopause — defined as 12 consecutive months without a menstrual period — both estrogen and progesterone levels remain permanently low.
Progesterone's role in hormone therapy
For women with an intact uterus who use estrogen therapy for menopausal symptoms such as hot flashes, night sweats, or vaginal dryness, progesterone (or another progestogen) is essential. Its primary role is to protect the uterine lining from excessive growth caused by estrogen alone, which could otherwise increase the risk of endometrial cancer.
Beyond uterine protection, research suggests progesterone may offer additional benefits:

• Promote a sense of calm
• Help preserve endothelial function during the menopause transition
• Contribute to increased bone mineral density when added to estradiol
Note: progesterone creams and other transdermal preparations do not provide adequate protection for the uterine lining and should not be relied upon for this purpose.
Understanding the terminology: progesterone vs. progestogens
Progestogens is the medical term for all hormones — natural or synthetic — that produce progesterone-like effects in the body. In menopause care, progestogens fall into two major categories:
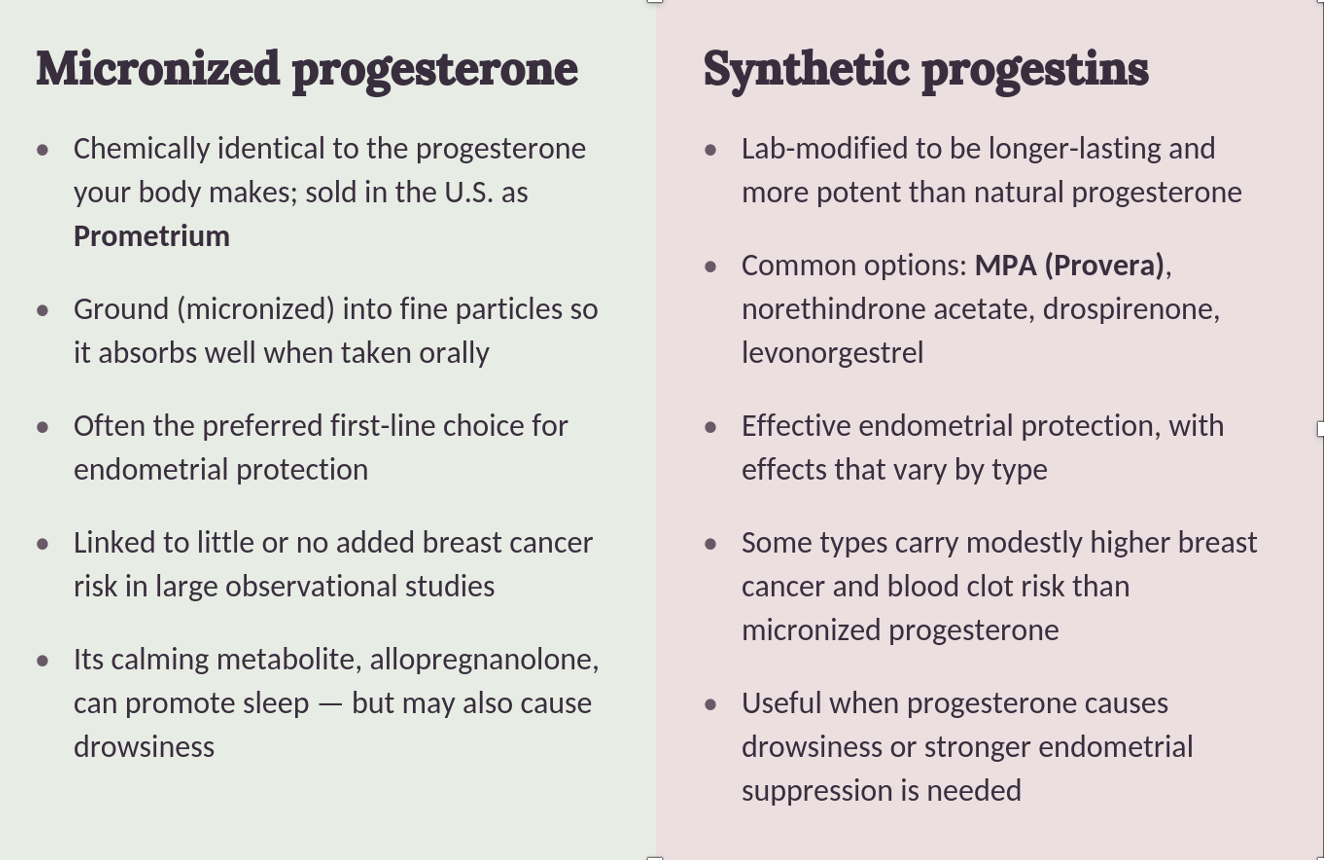
Micronized (bioidentical) progesterone: benefits and risks
Micronized progesterone is often considered the preferred first-line option for many women receiving menopausal hormone therapy. Its primary purpose is endometrial protection in women taking estrogen who still have a uterus. The hormone is micronized — ground into tiny particles — to improve absorption when taken orally.
Common dosing
• Sequential (cyclic): 200 mg daily for 12–14 days per month
• Continuous: 100 mg daily
Potential advantages
Favorable breast health profile — little or no impact on breast cancer risk when used with estrogen
Large observational studies suggest micronized progesterone may have little or no impact on breast cancer risk when used with estrogen, unlike some older synthetic progestins.
Lower blood clot risk — minimal increase when paired with transdermal estradiol
When combined with transdermal estradiol (patches or gels), micronized progesterone does not appear to significantly increase the risk of venous blood clots.
Metabolic neutrality — doesn't undo estrogen's benefits
It generally does not interfere with estrogen's favorable effects on cholesterol or blood sugar levels.
Improved sleep — converted into a calming neurosteroid
Progesterone is converted into a neurosteroid called allopregnanolone, which has calming and sleep-promoting effects. Many women report improved sleep quality when taking it at bedtime.
Hot flash reduction — meaningful relief in clinical studies
Clinical studies have demonstrated meaningful reductions in hot flashes, particularly among women with more severe symptoms.
Potential side effects
• The same calming effect can cause drowsiness and dizziness in some women
• Other side effects might include headaches, bloating, or vaginal bleeding
• Peanut oil is used in certain formulations — important for those with peanut allergies
Synthetic progestins: benefits and risks
Synthetic progestins remain valuable treatment options and may be the better choice in certain situations.
Medroxyprogesterone acetate (Provera)
Provera is one of the most extensively studied progestins and effectively protects the uterine lining. However, research has linked it to:
• Modestly increased breast cancer risk
• Higher blood clot risk compared with some alternatives
• Possible negative effects on mood
• Partial reduction of estrogen's beneficial effects on cholesterol and blood vessels
Norethindrone acetate (NETA)
NETA is derived from testosterone and has mild androgenic (male hormone-like) properties. It offers strong endometrial protection but may:
• Increase acne
• Cause unwanted hair growth
• Increase breast cancer risk with prolonged use
• Modestly affect cholesterol profiles
Drospirenone (DRSP)
Drospirenone is a newer progestin that is closer to natural progesterone than other synthetic progestins. It has some unique advantages:
• May improve acne
• Can reduce bloating and water retention
• May modestly lower blood pressure
• Does not appear to negatively affect cholesterol
However, it should be used cautiously in women with kidney disease or those taking medications that increase potassium levels.
Levonorgestrel intrauterine system (hormonal IUD)
The levonorgestrel-releasing IUD provides excellent endometrial protection while minimizing whole-body hormone exposure, with reduced systemic side effects and long-lasting protection of up to 5 years. The main limitation is that insertion may be difficult for some women.
When might a synthetic progestin be preferred?
Although micronized progesterone is often the preferred starting choice, synthetic progestins may be appropriate when:
• A patient has a peanut allergy
• Breakthrough bleeding remains problematic
• Stronger endometrial suppression is needed
• Progesterone causes excessive drowsiness
• A combination hormone product would simplify treatment
• Hypertension or fluid retention makes drospirenone particularly attractive
A brief note about dydrogesterone
Dydrogesterone (brand name Duphaston) is widely used in Europe and Asia but is not currently available in the United States. It closely resembles natural progesterone and has demonstrated:
• Effective endometrial protection
• Low breast cancer risk in available studies
• Low blood clot risk
• No significant effects on blood pressure, cholesterol, blood sugar, or weight
Unlike micronized progesterone, it does not typically cause drowsiness, making it an attractive option where available.
Progestogens and breast cancer: what you should know
One of the most common concerns women have about hormone therapy is breast cancer — and it's an important topic to understand. Not all progestogens carry the same level of risk. The large WHI study, which used a synthetic progestin called MPA (medroxyprogesterone acetate), found a small increase in breast cancer risk with combined estrogen-plus-MPA therapy after about 5 years of use.
However, multiple large European studies — including the landmark French E3N study, which followed more than 80,000 postmenopausal women — have consistently shown that micronized (bioidentical) progesterone and dydrogesterone are associated with significantly lower breast cancer risk than synthetic progestins.
Progesterone intolerance
About 30% of women find that the progesterone or progestin in their hormone therapy causes symptoms that feel a lot like PMS — bloating, breast tenderness, mood swings, irritability, headaches, or feeling weepy and anxious. This is known as progesterone intolerance, and it happens not because hormone levels are abnormal, but because some women's brains and bodies are simply more sensitive to progesterone's effects. The good news is that there are many ways to manage it:
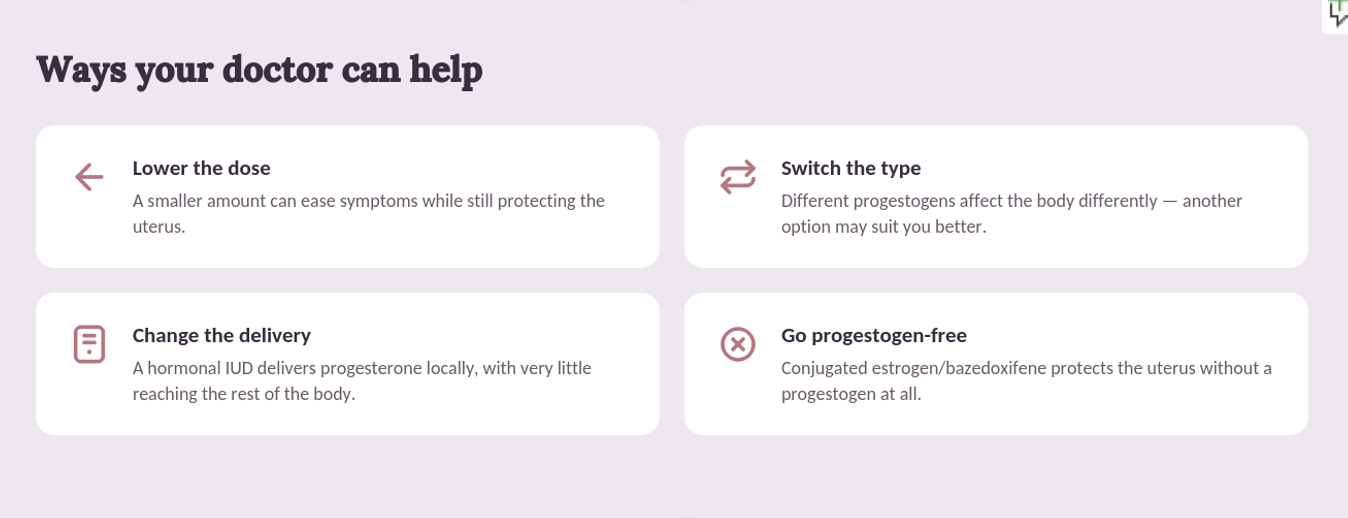
If you're experiencing these symptoms, don't just stop your therapy — talk to your provider, because there is almost always a better-tolerated alternative.
Bottom line
Progesterone is much more than a hormone added to protect the uterus. It plays an important role in sleep, mood, bone health, and overall hormonal balance. For many women considering menopausal hormone therapy, micronized (bioidentical) progesterone is often the preferred first-line option because of its favorable safety profile and sleep-promoting benefits.
That said, hormone therapy should always be individualized. Synthetic progestins remain important and appropriate options for women who cannot tolerate micronized progesterone or who have specific clinical needs. The best choice depends on your medical history, treatment goals, symptom profile, and personal preferences.
As always, discuss the risks and benefits of any hormone therapy with a qualified healthcare professional who can help determine the most appropriate option for you.
Key takeaways
1. Progesterone is typically the first hormone to decline during perimenopause, often well before estrogen drops.
2. Beyond uterine protection, progesterone supports sleep, calm, and bone health.
3. Micronized (bioidentical) progesterone is chemically identical to your body's own hormone and is often the preferred first-line option.
4. Synthetic progestins differ from one another — and from micronized progesterone — in their effects on breast cancer risk, blood clots, mood, and metabolism.
5. Progesterone creams and other transdermal preparations do not adequately protect the uterine lining.
6. About 30% of women experience progesterone intolerance, but switching the dose, type, or delivery method almost always helps.
7. The right progestogen depends on your medical history, symptoms, and personal preferences — always a shared decision with your provider.
Up next in this series
Testosterone — The Overlooked Third Hormone
References:
1. Hitchcock CL, Prior JC. Oral Micronized Progesterone for Vasomotor Symptoms in Healthy Postmenopausal Women — A Placebo-Controlled Randomized Trial. Menopause, 2012.
2. Fournier A, Berrino F, Clavel-Chapelon F. Unequal Risks for Breast Cancer Associated with Different Hormone Replacement Therapies: Results from the E3N Cohort Study. Breast Cancer Research and Treatment, 2008.
3. Fournier A, Mesrine S, Dossus L, et al. Risk of Breast Cancer After Stopping Menopausal Hormone Therapy in the E3N Cohort. Breast Cancer Research and Treatment, 2014.
4. Stute P, Wildt L, Neulen J. The Impact of Micronized Progesterone on Breast Cancer Risk: A Systematic Review. Climacteric, 2018.
5. Nolan BJ, Liang B, Cheung AS. Efficacy of Micronized Progesterone for Sleep: A Systematic Review and Meta-Analysis of Randomized Controlled Trial Data. Journal of Clinical Endocrinology & Metabolism, 2021.
6. Manson JE, Crandall CJ, Rossouw JE, et al. The Women's Health Initiative Randomized Trials and Clinical Practice: A Review. JAMA, 2024.
7. Stanczyk FZ. All Progestins Are Not Created Equal. Steroids, 2003.
8. British Menopause Society, IMS, EMAS, RCOG, and AMS. Joint Statement on Menopausal Hormone Therapy and Breast Cancer Risk, 2020.