
Menopause Hormones 101 — Part One Estrogen: the multitasker behind menopause
One hormone, dozens of jobs — and what changes in your body when it starts to fade.
Welcome to our Menopause Hormone 101 series. We're starting with Estrogen — the hormone most people associate with menopause. Estrogen plays a vital role in brain function, bone strength, heart health, mood, and metabolism, and declining levels are responsible for many common menopausal symptoms. Stay tuned for our next installment, Progesterone, where we'll explore estrogen's important hormonal partner.
What is estrogen, and why does it matter?
Estrogen isn't one molecule — it's a family of four related hormones, each playing a different role depending on your life stage.
Estradiol (E2) The lead — your reproductive years
The strongest and most important estrogen during your reproductive years. Produced mainly by the ovaries, it regulates your menstrual cycle, keeps bones strong, protects blood vessels, and supports brain and mood.
Estrone (E1) The understudy — after menopause
A weaker estrogen. After menopause, when the ovaries slow down, estrone becomes the main estrogen in your body — produced in fat tissue, where an enzyme called aromatase converts adrenal hormones into estrone.
Estriol (E3) The supporting role — pregnancy
The weakest estrogen. It's produced in large amounts during pregnancy but plays only a minor role at other times of life.
Estetrol (E4) The fourth estrogen — pregnancy
Sometimes called the “fourth estrogen,” estetrol is a natural estrogen made only by the fetal liver during pregnancy — your baby actually produced it while you were pregnant! Scientists have recently rediscovered E4 and are now studying it as a promising new option for both birth control and menopause treatment, because it appears to be gentler on the liver and breast tissue than other estrogens.
During perimenopause (the years leading up to your last period), estradiol levels fluctuate wildly — sometimes surging higher than normal, sometimes crashing. This hormonal roller coaster is what causes many of the symptoms women experience. After menopause, estradiol drops to very low levels permanently.
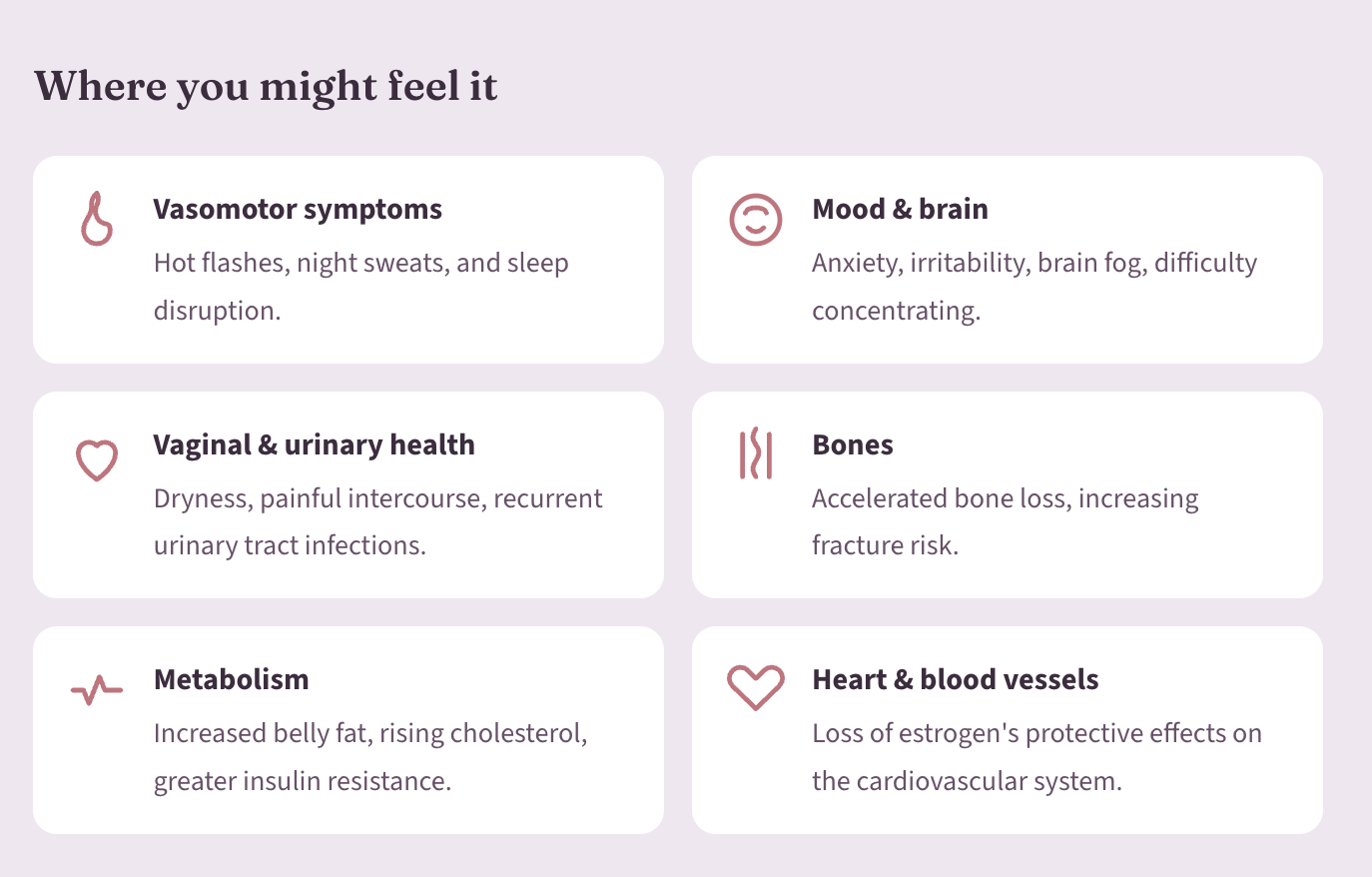
What happens when estrogen declines?
The effects of estrogen loss go far beyond hot flashes. Estrogen receptors exist in nearly every organ in your body — so when levels fall, changes can show up almost anywhere.
Short-term benefits: symptom relief
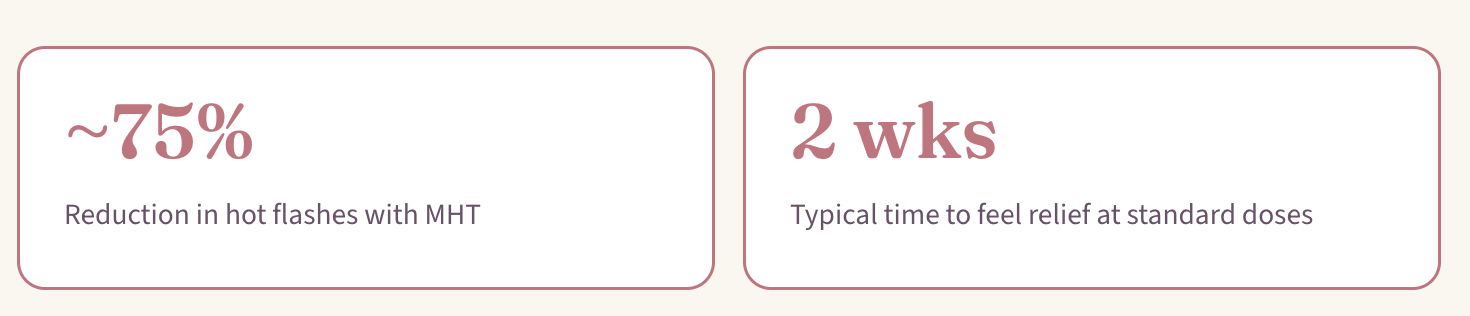
The most immediate reason women consider hormone therapy is symptom relief. Menopausal hormone therapy (MHT) is the most effective treatment available for vasomotor symptoms — and relief typically begins within two weeks at standard doses.
MHT also effectively treats:
Night sweats and related sleep problems
Vaginal dryness and painful intercourse
Mood swings and irritability related to hormonal changes
For women whose only symptom is vaginal dryness or discomfort, low-dose vaginal estrogen (creams, rings, or inserts) can be used locally with very little absorption into the rest of the body — making it safe for a much wider group of women.
Long-term benefits: bones, metabolism, and heart
Beyond symptom relief, estrogen has important effects on long-term health. These benefits are most relevant when hormone therapy is started early — around the time of menopause.
Bone health
Estrogen is essential for maintaining bone density. After menopause, bone loss accelerates significantly, and the risk of osteoporosis and fractures rises. In the Women's Health Initiative (WHI), the largest study of menopausal hormone therapy, estrogen therapy significantly reduced the risk of fractures.
WHI study: −388 Fewer fractures (including hip fractures) per 10,000 women over ~7 years
Metabolic health
Menopause is associated with increased belly fat, rising cholesterol, and greater insulin resistance — all of which raise the risk of type 2 diabetes and heart disease. Studies show that hormone therapy can improve insulin sensitivity and reduce the incidence of new-onset type 2 diabetes and has also been shown to reduce abdominal fat accumulation and improve lean body mass.
WHI study: −134 Fewer new cases of type 2 diabetes per 10,000 women over ~7 years
Heart health and the "window of opportunity"
The relationship between estrogen and heart health is one of the most discussed topics in women's health.
Estrogen is not recommended as a treatment to prevent heart disease.
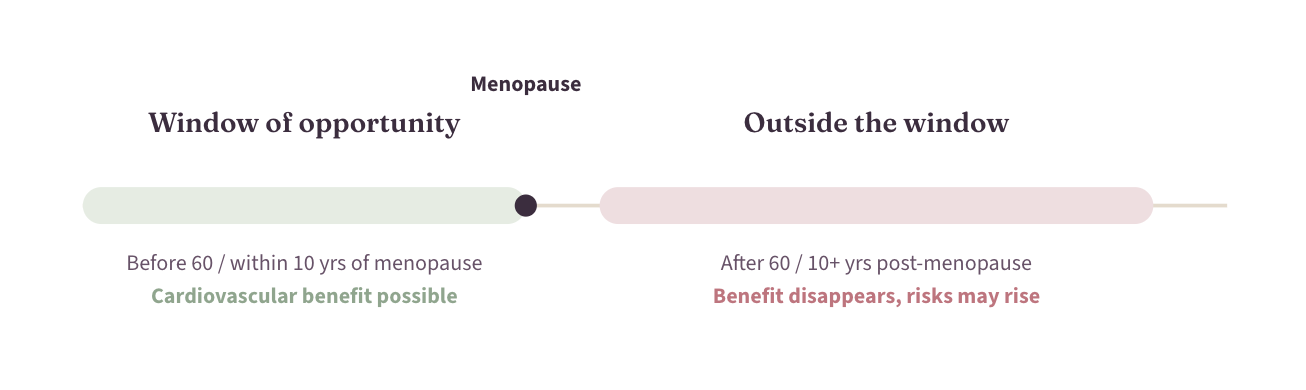
However, when hormone therapy is started before age 60 or within 10 years of menopause, studies suggest it may reduce the risk of coronary heart disease by roughly 50% and all-cause mortality by about 30%, compared to women who don't use it — known as the "timing hypothesis" or "window of opportunity."
When hormone therapy is started after age 60 or more than 10 years past menopause, these benefits disappear, and the risks of heart attack, stroke, and blood clots may increase.
Transdermal estrogen (patches, gels, sprays) may be safer for the heart and blood vessels than oral estrogen pills, because it avoids the liver's "first-pass" effect, which can increase clotting factors.
The bottom line: timing matters. Starting hormone therapy around the time of menopause appears to be the safest and most beneficial approach for cardiovascular health.
Types of estrogen used in menopause hormone therapy
Not all estrogen products are the same. Here's a quick guide.
Transdermal estradiol (patches, gels, sprays)
A bioidentical form of estrogen (chemically identical to what your body makes), delivered through the skin and avoiding the liver. Currently considered the first-line option by many experts for its convenience and potentially improved safety profile. Common brands: Climara, Vivelle-Dot, Divigel, Estrogel.
Oral estradiol (pills)
Also, bioidentical. Common brand: Estrace.
Conjugated equine estrogens (CEE)
Derived from horse urine (brand name Premarin). This was the estrogen used in the WHI study and contains a mix of estrogens, not just estradiol.
Vaginal estrogen — low dose (local therapy)
Creams, low-dose rings, and tablets/inserts that act locally in the vagina and urinary tract to treat Genitourinary Syndrome of Menopause (GSM). Very little gets into the bloodstream — safe for a wide range of women, including many over age 60 and even some breast cancer survivors (in consultation with an oncologist).
Vaginal estrogen — higher dose (systemic therapy)
A higher-dose estradiol vaginal ring (brand name Femring) is designed to deliver enough estrogen through the vaginal wall to treat systemic symptoms, not just local ones — a convenient option for women who prefer not to take pills or wear patches.
If you have a uterus, you'll also need progesterone or a progestin along with estrogen to protect the lining of your uterus from overgrowth. Micronized progesterone (brand name Prometrium) is the bioidentical option and may have a better safety profile than synthetic progestin. Stay tuned for our blog about progesterone to learn more.
How is estrogen in birth control pills different from MHT?
This is a common and important question. While both birth control pills and MHT contain estrogen, they are quite different.
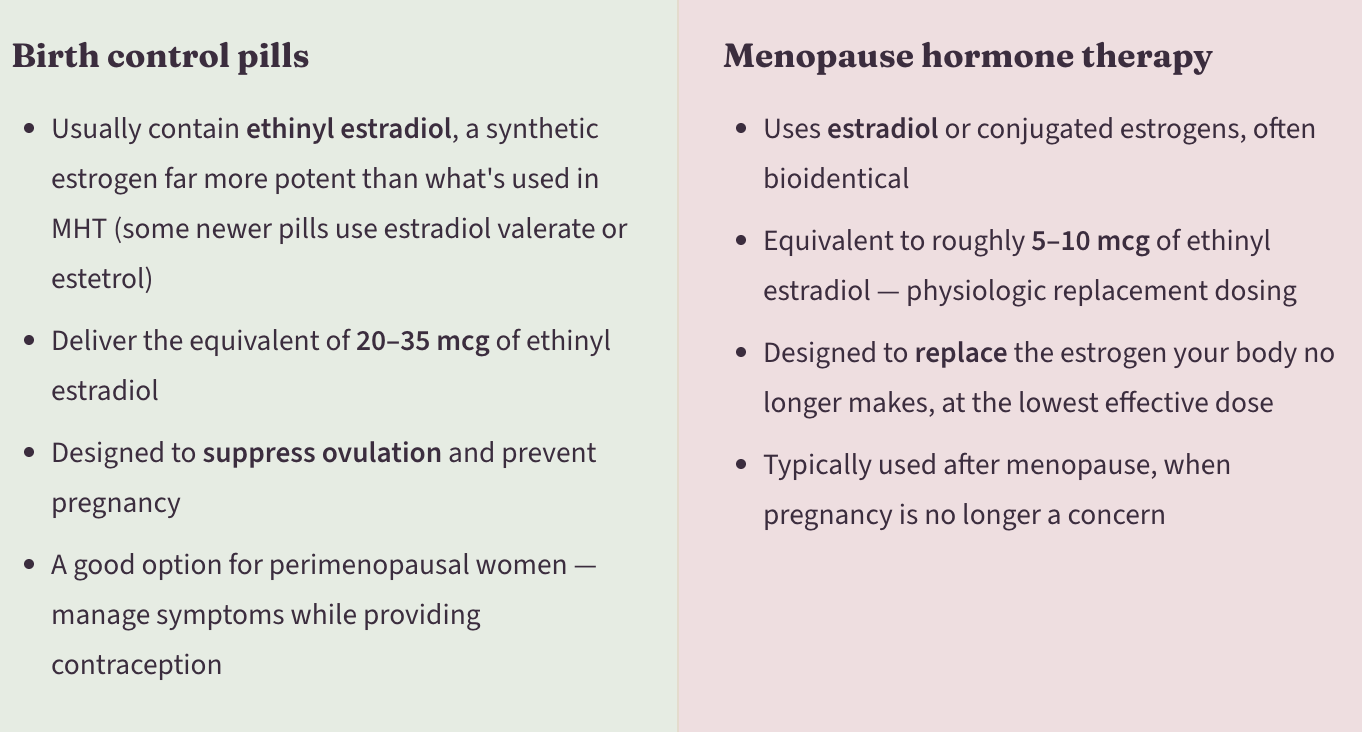
ACOG and The Menopause Society both support continuing hormonal birth control until age 50–55 in healthy women without contraindications, then transitioning to MHT if symptoms persist.
Think of it this way Birth control pills use a higher dose of a stronger synthetic estrogen to shut down your ovaries. MHT uses a lower dose of a gentler, often bioidentical estrogen to replace what your ovaries have stopped making.
Is hormone therapy safe? What about breast cancer?
This is the question that worries women the most — and the one where the science has changed the most in recent years.
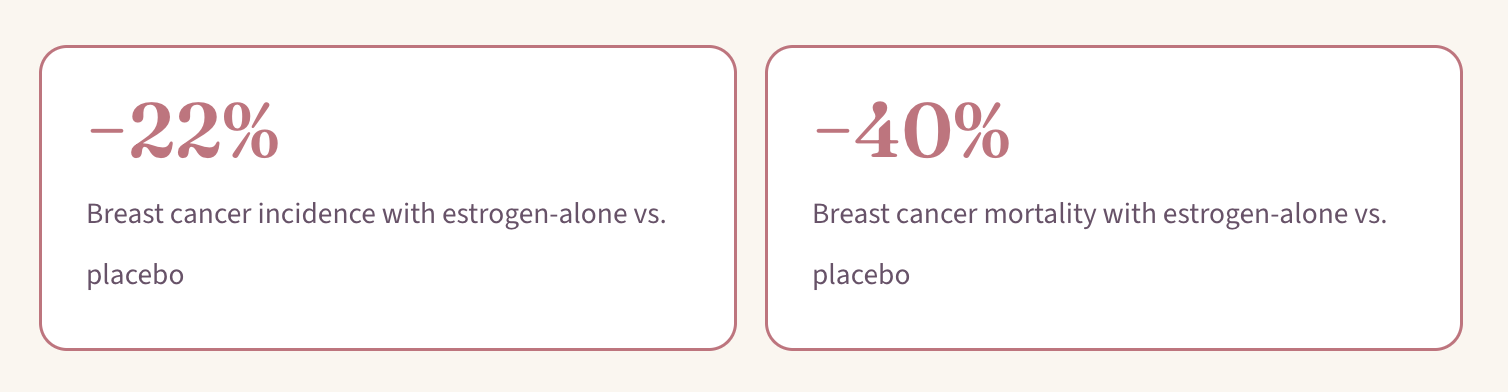
Estrogen alone does not increase breast cancer risk. In the WHI — the largest and longest randomized trial of hormone therapy — women who took estrogen alone (without a progestin) had a significantly lower risk of developing breast cancer and a significantly lower risk of dying from breast cancer compared to women who took a placebo. A 2024 meta-analysis of all 10 randomized trials of estrogen alone confirmed this finding.
Emerging research suggests it's the progestogen (progesterone or progestin) component — not the estrogen — that's the primary driver of the small increase in breast cancer risk seen with combined hormone therapy.
Combined estrogen + progesterone therapy (needed for women who still have a uterus) does carry a small, duration-dependent increase in breast cancer risk. In the WHI, which used a synthetic progestin called medroxyprogesterone acetate (MPA), this increase became apparent after about 5 years of use. However, the absolute risk is small — roughly 1 additional case per 1,000 women per year of use, similar to the risk associated with obesity, physical inactivity, or drinking one alcoholic beverage daily. The type of progestogen matters: micronized progesterone appears to have a more favorable breast safety profile than synthetic progestins like MPA, though this hasn't been confirmed in large, randomized trials.
For most healthy women under 60 who are within 10 years of menopause, the benefits of hormone therapy generally outweigh the risks. That said, hormone therapy is not right for everyone. It should be avoided in women with:
· A history of breast cancer (although there are exceptions)
· A history of other estrogen- sensitive cancers
· A history of heart attack or angina
· A history of blood clots or strokes
· Active liver disease
· Unexplained vaginal bleeding
Every woman's situation is different. The decision to use hormone therapy should be a shared one between you and your healthcare provider, weighing your specific symptoms, health history, and personal preferences.
Key takeaways
1. Estrogen decline during perimenopause and menopause affects far more than your periods — it impacts your bones, heart, brain, metabolism, and quality of life.
2. Menopausal hormone therapy is the most effective treatment for hot flashes and other menopausal symptoms.
3. Starting hormone therapy early (before age 60 or within 10 years of menopause) offers the best balance of benefits and risks.
4. Transdermal estrogen (patches, gels) is often preferred over pills for its safety profile.
5. Estrogen can be delivered orally, through the skin, or vaginally — and vaginal estrogen comes in both low-dose (local) and higher-dose (systemic) forms.
6. Birth control pills and MHT are not the same — they use different types and doses of estrogen for different purposes.
7. Long-term, estrogen helps protect your bones from fractures, improves insulin sensitivity, and may support heart health when started at the right time.
Up next in this series
Progesterone — Estrogen's Essential Partner
References:
1. Chlebowski RT, Anderson GL, Aragaki AK, et al. Association of Menopausal Hormone Therapy With Breast Cancer Incidence and Mortality During Long-term Follow-up of the Women's Health Initiative Randomized Clinical Trials. JAMA, 2020.
2. Manson JE, Crandall CJ, Rossouw JE, et al. The Women's Health Initiative Randomized Trials and Clinical Practice: A Review. JAMA, 2024.
3. Chlebowski RT, Aragaki AK, Pan K, et al. Randomized Trials of Estrogen-Alone and Breast Cancer Incidence: A Meta-Analysis. Breast Cancer Research and Treatment, 2024.
4. Gompel A, Simcock R. Menopausal Hormone Treatment and Breast Cancer. The Lancet Diabetes & Endocrinology, 2026.
5. Crandall CJ, Mehta JM, Manson JE. Management of Menopausal Symptoms: A Review. JAMA, 2023.
6. El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention. Circulation (American Heart Association), 2020.
7. Hodis HN, Mack WJ, Henderson VW, et al. Vascular Effects of Early versus Late Postmenopausal Treatment with Estradiol. New England Journal of Medicine, 2016.
8. Sriprasert I, Hodis HN, Mack WJ, et al. Elimination of the Black Box Warning on Menopausal Hormone Therapy. Obstetrics & Gynecology, 2026.
9. Pinkerton JV, Simon JA, Hodis HN, et al. Report of the FDA's Expert Panel on Hormone Therapy. Menopause, 2026.
10. Gartlehner G, Patel SV, Reddy S, et al. Hormone Therapy for the Primary Prevention of Chronic Conditions in Postmenopausal Persons. JAMA (US Preventive Services Task Force), 2022.
11. Bartz D, Tadikonda A, Manson JE. Opportunity for Improved Menopausal Hormone Therapy Prescribing. JAMA, 2026.