
Nutrition, Sleep, and Medical Therapies for Menopausal Belly Fat (Belly Fat series, #4)

While exercise is foundational, it is only one part of the equation when it comes to addressing belly fat in menopause. The physiologic changes driven by declining estrogen affect metabolism, appetite regulation, fat storage, and energy balance. This means that nutrition, sleep, and targeted medical therapies all play critical roles in achieving meaningful and sustainable improvements in body composition.
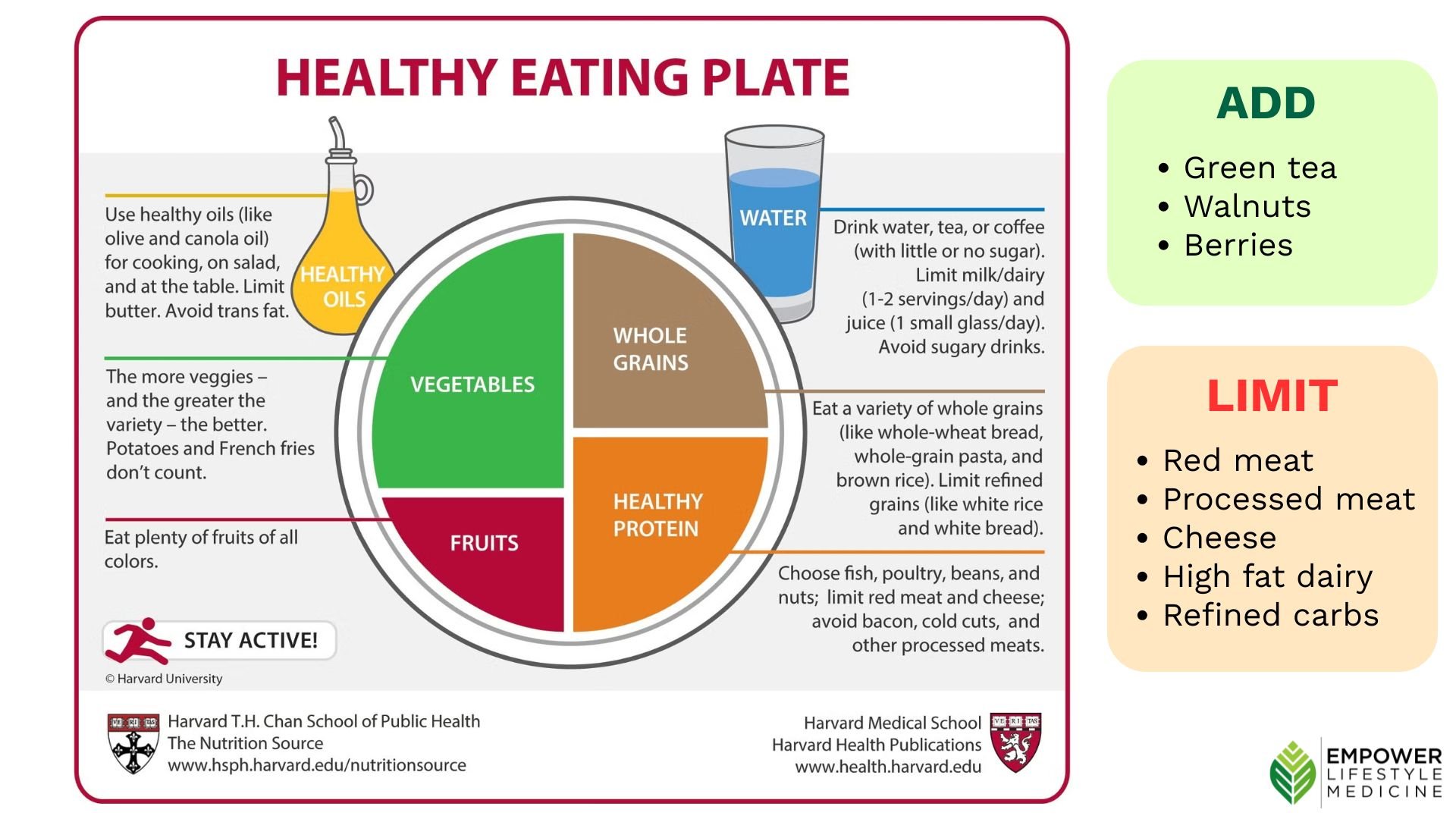
Nutrition: Why a High-Polyphenol, Plant-Predominant Diet Matters
A growing body of evidence supports a dietary pattern that is rich in plant-based foods and particularly high in polyphenols—bioactive compounds found in plants that have powerful metabolic effects.
Polyphenols are not just “antioxidants” in a general sense. They exert multiple biologic actions that are directly relevant to menopause-related fat gain. These include:
Improving insulin sensitivity
Reducing inflammation
Decreasing cholesterol absorption
Lowering blood pressure
Influencing fat metabolism and storage
These mechanisms are especially important in menopause, where insulin resistance and inflammation tend to increase.
One of the most compelling pieces of evidence comes from a study comparing different dietary patterns, including a standard healthy diet, a calorie-restricted Mediterranean diet low in refined carbs, and a “Green Mediterranean” diet—a version of the Mediterranean diet specifically enriched in polyphenols.
In this study, participants following the higher-polyphenol dietary pattern achieved greater reductions in visceral fat (14%) compared to participants following a standard healthy diet (4%) and participants following the calorie-restricted Mediterranean diet (6%). The key differences in the high-polyphenol group included:
Increased intake of green tea (3–4 cups daily)
Inclusion of polyphenol-rich plant sources
Avoidance of red and processed meats
This suggests that what you eat—not just how much—directly influences where fat is stored.
Foods Rich in Polyphenols
Incorporating polyphenol-rich foods into your daily routine can meaningfully impact metabolic health. High-polyphenol foods include:
Berries (blueberries, strawberries, raspberries)
Leafy greens and vegetables
Nuts and seeds (especially walnuts and flaxseed)
Spices and herbs (especially cloves, oregano, mint)
Cocoa
Green and black tea
These foods not only support fat loss but also improve cardiovascular and metabolic health—making them particularly valuable during menopause.
Protein and Fiber: Foundational Targets
Beyond polyphenols, two additional nutritional priorities are essential:
Protein: Aim for ~0.6–0.8 g per lb of ideal body weight
Adequate protein intake supports muscle preservation, which is critical for maintaining metabolic rate during menopause. Choose lean proteins, and prioritize plant-based sources over animal sources. Good sources of lean protein include beans, soy milk, extra firm tofu, tempeh, fish, chicken breast, non-fat dairy such as Greek yogurt.Fiber: Aim for 30–38 g daily
Fiber improves satiety, supports the gut microbiome, reduces cholesterol, and enhances insulin sensitivity. Good sources include beans, whole fruit, vegetables, whole grains, seeds and nuts.
Limiting refined carbohydrates, red and processed meats, and high-fat dairy products (such as cheese and butter) is also important, as these are associated with increased visceral fat.
Putting it all together – the nutrition plan for reducing belly fat in menopause.
Sleep: A Hidden Driver of Belly Fat
Sleep disruption is one of the most underappreciated contributors to weight gain in midlife.
Hormonal changes during menopause frequently lead to insomnia, fragmented sleep, or reduced sleep quality. These changes have direct metabolic consequences.
When sleep is insufficient or disrupted:
Ghrelin (hunger hormone) increases
Leptin (satiety hormone) decreases
Daily calorie intake increases—often by 250 calories or more
In addition, poor sleep:
Reduces insulin sensitivity
Increases cortisol (a stress hormone that promotes abdominal fat storage)
Impairs decision-making around food choices
Over time, these changes create a biologic drive toward weight gain, particularly in the abdominal region.
Addressing Sleep: CBT-I
Cognitive Behavioral Therapy for Insomnia (CBT-I) is considered first-line treatment and focuses on:
Sleep hygiene (consistent schedule, dark/cool environment)
Stimulus control (associating the bed only with sleep)
Sleep restriction (aligning time in bed with actual sleep time)
Relaxation techniques and meditation
Improving sleep is not just about feeling better—it is a critical step in improving metabolic health and reducing belly fat.
Hormone Therapy: Addressing the Root Cause
Because estrogen decline is a key driver of menopausal body composition changes, it makes sense that replacing estrogen—when appropriate—can improve these outcomes.
Menopausal hormone therapy (MHT), which includes estrogen alone or in combination with progesterone, has been shown to have measurable metabolic benefits.
In studies assessing body composition using DEXA scans, women using hormone therapy had lower levels of abdominal fatand visceral fat with age compared to those not using therapy.
A large meta-analysis of over 100 clinical trials demonstrated that MHT is associated with:
~7% reduction in abdominal fat
~13% reduction in insulin resistance
~16% improvement in LDL/HDL cholesterol ratio
Modest reductions in blood pressure
These findings highlight that estrogen is not only a reproductive hormone—it is a metabolic regulator that influences fat distribution, insulin sensitivity, and cardiovascular risk.
Of course, hormone therapy is not appropriate for everyone, and decisions should be individualized based on medical history, risk factors, and goals. But for many women, it can be a powerful tool in addressing both symptoms and metabolic health.
GLP-1 Medications: A Powerful Tool for Metabolic Health
GLP-1 receptor agonists are an increasingly important option in the treatment of overweight and obesity, particularly in individuals who struggle to achieve results with lifestyle interventions alone.
These medications work by mimicking the hormone GLP-1, which:
Slows gastric emptying
Enhances satiety (feeling full)
Reduces appetite
Improves insulin secretion and glucose regulation
The result is a reduction in overall calorie intake and meaningful weight loss.
In the context of menopause—where appetite regulation and insulin sensitivity are often disrupted—GLP-1 medications can help counteract these physiologic changes.
They are typically considered for individuals with:
A BMI ≥ 27 with co-morbidities such as elevated cholesterol markers, hypertension, arthritis, or insulin resistance
Or a BMI ≥ 30
Beyond weight loss, GLP-1 medications also:
Improve glycemic control
Reduce cardiovascular risk
Support long-term metabolic health
They are not a replacement for lifestyle changes—but rather a tool that can enhance and support them.
Additional Support: Creatine
Creatine supplementation (3–5 g daily) can be particularly beneficial when combined with resistance training.
Creatine has been shown in many studies to:
Increase muscle mass
Improve strength and exercise performance
May contribute to modest reductions in fat mass
Given the importance of muscle preservation during menopause, creatine is a simple and evidence-based addition for many women.
The Bottom Line
Menopausal belly fat is not caused by a single factor—and it cannot be addressed with a single solution.
It is the result of overlapping changes in:
Hormones
Body composition
Metabolism
Behavior (sleep, nutrition, activity)
The most effective approach is therefore comprehensive and targeted:
A high-polyphenol, plant-predominant diet
Adequate protein and fiber intake
Consistent, restorative sleep
Strategic use of exercise
Consideration of hormone therapy and medications when appropriate
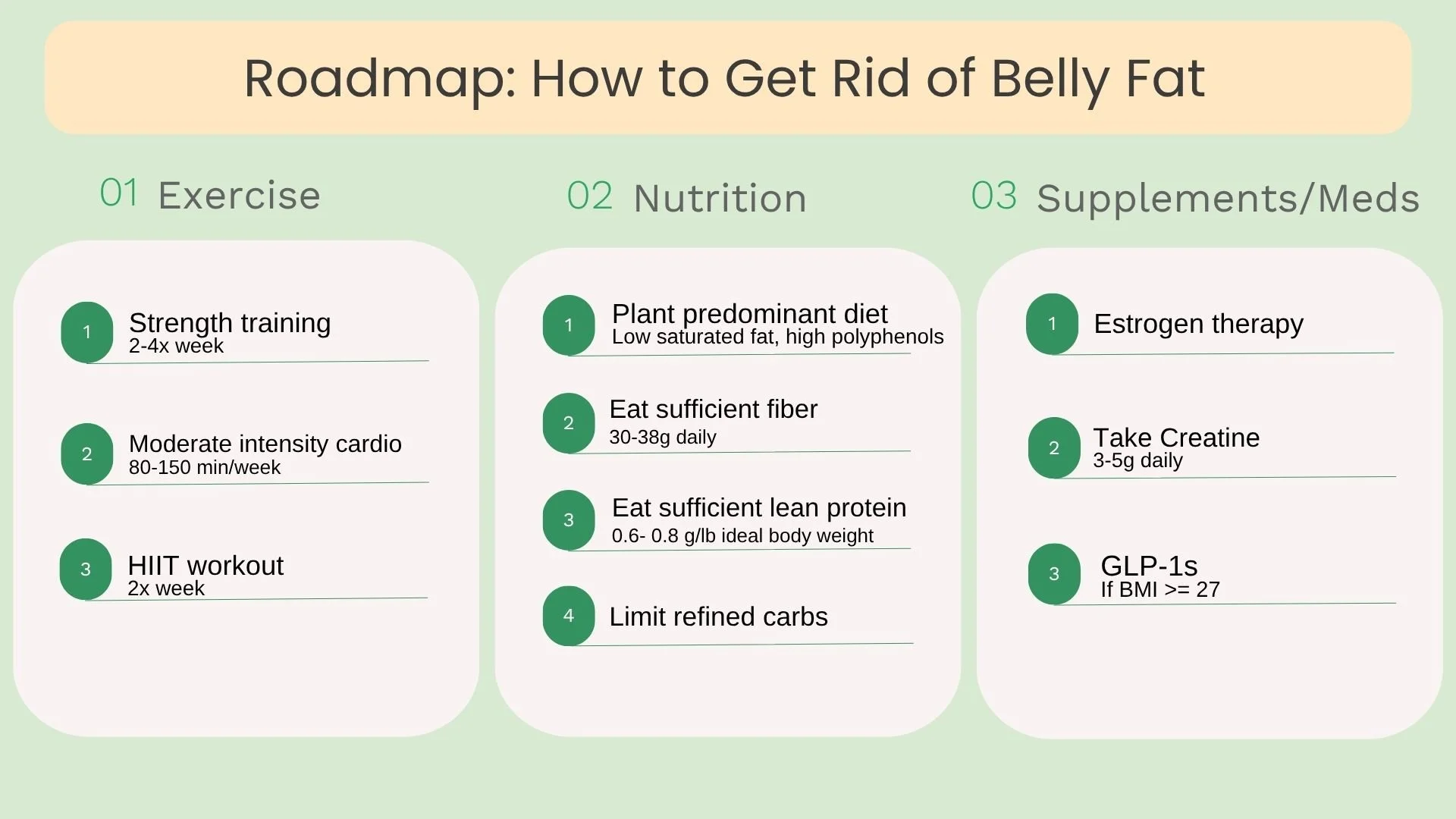
Putting it all together: Exercise, nutrition, +/- hormone therapy, creatine supplementation, and +/- GLP-1 medication.
This is not about fighting your body—it’s about understanding the physiologic changes of menopause and using that knowledge to your advantage.
References:
Zelicha H, et al. The effect of high-polyphenol Mediterranean diet on visceral adiposity: the DIRECT PLUS randomized controlled trial. BMC Med. 2022 Sep 30;20(1):327.
Papadakis GE, et al. Menopausal Hormone Therapy Is Associated With Reduced Total and Visceral Adiposity: The OsteoLaus Cohort. J Clin Endocrinol Metab. 2018 May 1;103(5):1948-1957.
Salpeter SR, et al. Meta-analysis: effect of hormone-replacement therapy on components of the metabolic syndrome in postmenopausal women. Diabetes Obes Metab. 2006 Sep;8(5):538-54.
Chaput JP, et al. The role of insufficient sleep and circadian misalignment in obesity. Nat Rev Endocrinol. 2023 Feb;19(2):82-97.